In the announcement about Kate Spade’s suicide in the New York Times, Mr. Spade said:
that though his wife had suffered from anxiety at points during their relationship and marriage, her serious bouts of depression only began about six years ago, at the age of 49.
Kate suffered from depression and anxiety for many years. She was actively seeking help and working closely with her doctors to treat her disease, one that takes far too many lives. We were in touch with her the night before and she sounded happy. There was no indication and no warning that she would do this. It was a complete shock. And it clearly wasn’t her. There were personal demons she was battling.
My heart goes out to Kate Spade’s husband, young daughter and loved ones. Her suicide is just so sad but as I said I have a fair bit to say about this….
Hormone imbalance triggering anxiety and depression?
According to the reports, Kate’s “serious bouts of depression only began about six years ago, at the age of 49, but she had suffered “from depression and anxiety for many years”.
Perimenopause and menopause is a classic time for women to experience worsening anxiety and depression and can be driven by fluctuating hormones, especially low estrogen. In this study, Depression and the menopause: why antidepressants are not enough? the authors share that
Postmenopausal depression is more severe, has a more insidious course, is more resistant to conventional antidepressants in comparison with premenopausal women and has better outcomes when antidepressants are combined with HT (hormone therapy).
Addressing hormone imbalance as one possible root cause can eliminate the anxiety and depression. Some of my favorite resources for hormone balance are these books: The Hormone Secret and Cooking for Hormone Balance.
Low levels of neurotransmitters like serotonin, catecholamines and GABA?
Directly connected to hormonal imbalance is brain chemistry imbalance. Addressing low levels of neurotransmitters like serotonin, the catecholamines and GABA provide results quickly when they are used in a targeted way based on individual needs:
- Low serotonin is an issue when estrogen levels are declining and the amino acid tryptophan can have profound benefits if low serotonin is one of the root causes, leading to depression, worry, fear, overwhelm and sleep issues.
- Low catecholamines can cause the “I just want to say in bed” depression and low motivation, together with fatigue and poor focus. The amino acid tyrosine can help to eliminate some of this and also provides thyroid support. Poor thyroid health can also be a root cause of depression.
- We see low GABA levels when progesterone is low and if this is one of the root causes, it can result in increased physical anxiety and insomnia. The amino acid GABA, opened on to the tongue, can provide calming results within minutes.
I can totally relate to the hormonal aspect as I suffered from PMS for years and my anxiety issues and panic attacks started in my late 30s and I had a really low spell as I was going through menopause. Both GABA and tryptophan turned things around very quickly for me as they do for my clients.
The role of diet and nutritional psychiatry?
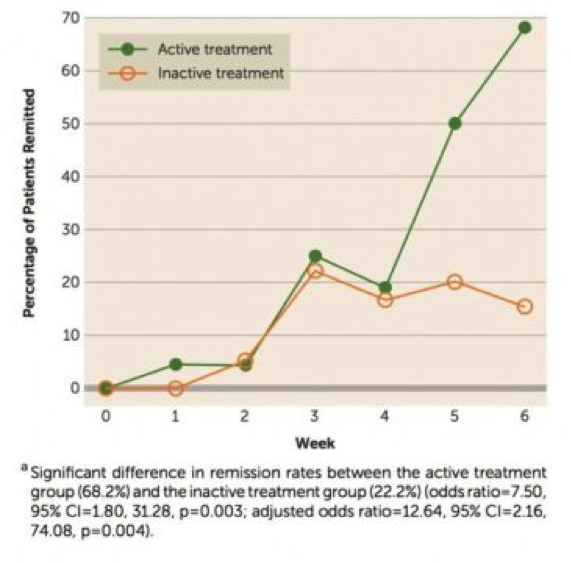
There is so much new science behind the role of a real foods traditional diet for alleviating both depression and anxiety. The SMILES study, published by Prof Felice Jacka early 2017, was the first randomized controlled diet depression study and ONE THIRD of the dietary intervention group saw improvements in their depression symptoms. This was just diet alone and switching from processed and junk food to real food with no specific dietary restrictions.
There is also much clinical evidence supporting how diet can have an impact. Holly, suffered from with severe depression and anxiety changed her diet and shared this with me:
Over the course of a year and a half, I was given 10 different psychiatric diagnoses and cycled through 10 different medications. I discovered the healing power of diet completely by accident, and it changed my life. I now live with no diagnoses and no symptoms.
I started with the Whole30 (strict paleo), then went paleo, dabbled with a ketogenic approach, and now I eat a modified paleo diet, with some rice and goat dairy.
This has been termed nutritional psychiatry and you can read more diet-depression and diet-anxiety success stories here.
Keep in mind that your prescribing psychiatrist may not yet be on board with this or up to date on the newest research. Just last week someone told me what happened when they discussed nutritional psychiatry with their doctor and showed them my book The Antianxiety Food Solution (my Amazon link). He said: “Good luck with that!”
Could the antidepressant medication have triggered her suicide?
The statement from Kate’s husband says “She was actively seeking help for depression and anxiety over the last 5 years, seeing a doctor on a regular basis and taking medication for both depression and anxiety.” Could the antidepressant medication have triggered her suicide or played some part?
We will never know with Kate but this is always my first thought when I learn of a suicide and when we hear of homicides in the news. One of my colleagues shared this when her suicide was first announced: “I was wondering if she was under psych care and what role meds might have played in this tragedy.”
This paper is one of many papers reporting similar antidepressant suicide and violence risks, and concludes that:
Antidepressants double the occurrence of events in adult healthy volunteers that can lead to suicide and violence
Kelly Brogan MD – Holistic Psychiatrist no longer prescribes psychiatric medications because we don’t know who will experience this side-effect. She writes this about a Swedish study and antidepressants and increased suicides
As antidepressant prescriptions increased 270% over 15 years, suicide rates also increased. Strikingly, more than half of the young women who committed suicide (52%) were prescribed antidepressants within a year of committing suicide. And antidepressants were detected in 41% of the women who committed suicide, showing that they were under the influence of antidepressants at the time of death.
What if you are taking an antidepressant and seeing benefits?
When I posted some of this on Facebook earlier in the week someone who is on an antidepressant and benefiting shared her frustration that we are blaming suicide on medications.
There are many who do benefit but there are two issues I have:
- Even if someone is doing well on an antidepressant, benzodiazepine or other psychiatric medication I feel we need informed consent about the side-effects and training for the individual and family on what to look out for as things can change. The can occur when meds are changed, doses are increased or decreased, new meds are added, one or more are stopped abruptly or too quickly (called discontinuation syndrome). Many doctors also need to be educated and to acknowledge that suicide and homicide are very real side-effects of these meds.
- We don’t know who will be adversely impacted, which is why consent/knowledge about this is so important.
When we rent ski equipment or go bungee jumping we sign an informed consent form, acknowledging the possible risks of death. Why is this not happening with these medications? I just want individuals to be going into this with eyes wide-open so they don’t say “why didn’t anyone tell us this?”
If someone is currently seeing benefits from antidepressants (or benzodiazepines) I make sure they know ALL the risks and encourage them to continue to look for root the causes and address these (never stopping medications abruptly and never without the prescribing doctor’s permission).
There are many possible biological or biomedical or metabolic causes of depression and anxiety and many of these can play a factor in suicide. Here is a list of just some of them:
- gluten sensitivity and celiac disease
- low B12, low B6, low omega3s, low zinc
- the anti-malaria drug mefloquine (has been associated with acts of violence and suicide)
- toxoplasma gondii
- fluoroquinolone antibiotics
- many common drugs may be contributing to depression (over 200 including acid reflux meds, blood pressure meds, birth control pill)
My concern is that none of these – the medications or poor diet and nutritional deficiencies – are ever discussed when someone does commit suicide or goes on a violent or homicidal rampage.
The stigma of mental health and the fear of seeking help
There are reports that “Kate Spade felt unable to seek help or discuss her mental health because she feared this might damage the brand she created.” This is a huge issue and if it was true for her or if anyone with a mental health condition feels like this, this has to change!
As Dr. Mark Hyman MD said this when I interviewed him last year before the launch of his Broken Brain docu-series
I began to realize that the body was driving a lot of this brain dysfunction, and that if you fix the body, a lot of the brain disorders would get better, that it wasn’t a primarily a mental problem, but it was a physical problem.
Our interview and full transcript is here and we cover the gamut in 12 minutes: the gut and microbiome, nutritional deficiencies, food sensitivities, heavy metals, other environmental toxins and medications.
We don’t hide the fact that we have a broken leg so why do we have to hide it when we have a broken brain? If we can start to acknowledge that mental health issues so often have this physical aspect (and often it’s 100% physical) then hopefully we can end this crazy stigma.
And even if there is also trauma or lifestyle factors that make someone depressed or anxious – so be it. Stop the stigma and shame. Why do we have to put on a brave face and pretend all is well. It has to stop so people can ask for help.
Last but not least, I feel we need to offer practical nutritional psychiatry resources to the family who have been traumatized by the loss of a loved one to suicide. We know the amino acids and B vitamins help individuals recover from psychological stress after a natural disaster and these same nutrients can help the family in the midst of their sorrow.
I am aware it’s a very delicate subject and I’m sure this will rub some people the wrong way but I believe we all need to be talking about this and not tip-toeing around it.
I really feel this all needed to be said today. I hope this helps you or a loved one.
Rest in peace Kate Spade.