A very common question I get is from folks asking about the difference between the amino acids DPA (d-phenylalanine) and DLPA (dl-phenylalanine) for endorphin support and endorphin/dopamine support. I dedicate an entire blog to this question explaining the differences and which one I use for weepiness, heart-ache, pain and energy. I also discuss where tyrosine (for dopamine support) fits in. If you missed that or need a recap you can read about this on the blog.
The blog post generated some great questions that I’m sharing today, with my feedback, in case you have similar questions. I discuss a question about DLPA vs DPA for pain and impacts on sleep; a question about DLPA (used by mistake) raising already high dopamine levels and why DPA isn’t working any more for food cravings; a question about using DPA with GABA; and a question about DPA for depression and lack of joy caused by grief.
Here is the question from Gloria who shared this feedback about her use of DLPA (as part of a pain relief product) but says she can’t use it past noon. She also wants to know more about DPA for pain relief:
My experience with DLPA is as part of a supplement called Curamin for pain relief from arthritis that also has curcumin and boswellia. It works quite well in the AM but I can’t tolerate it past noon or it negatively affects my sleep.
Interesting to learn it is similar to tyrosine which I have had sleep problems with in the past.
Does DPA work as well for pain? Is it best to take amino acids on an empty stomach for best absorption? Does that mean an hour before a meal or two hours after? Thank you for your blogs and book!
It’s great that this combination product offers pain relief and it’s good that she has made the connection to poor sleep when it’s used after noon. This is a popular product that I would like to see include the possible impacts on sleep and the other precautions for DLPA . It is a proprietary formulation so you don’t actually know how much DLPA you’re getting. I really don’t like not knowing.
One other concern is that curcumin is high-oxalate and for some this can make pain worse. Otherwise, curcumin and boswellia are excellent for pain relief and reducing inflammation.
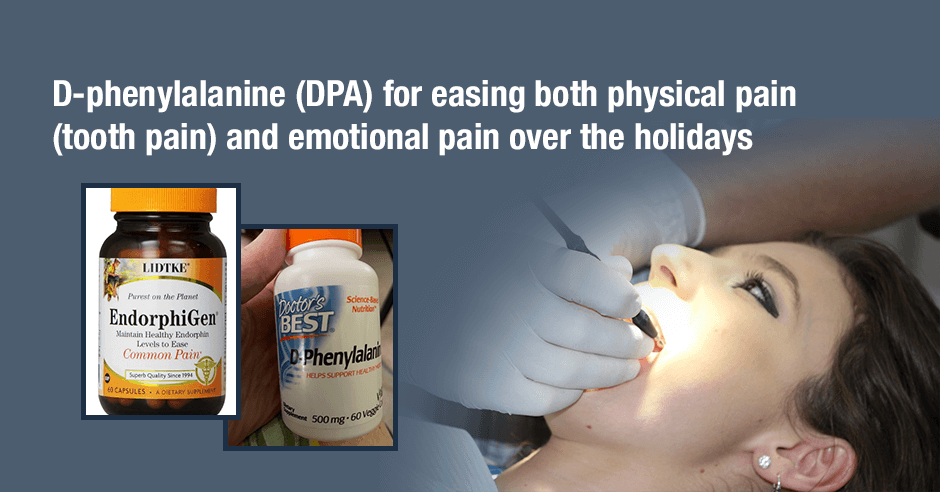
DPA is more effective for pain than DLPA because it offers a bigger endorphin boost. If oxalates are not an issue, one option could be to continue with the Curamin before noon and if needed, add standalone DPA in the afternoon and evening, for added pain relief.
Amino acids are more effective on an empty stomach and even more effective when opened on to the tongue. I share more about opening DPA onto the tongue in this blog.
DLPA (used by mistake) raised already high dopamine levels and why isn’t DPA working any more for food cravings?
Rhonda shared how she found out the difference between DPA and DLPA the hard way and wants to go back to DPA:
I certainly found out the difference the hard way. I had used Lidtke Endorphigen for a few years and I think it helped a bit with food cravings. As I am in Australia, I depend on my sister’s visits from US for my supply. When I ran out last year, I bought DLPA by mistake.
After 1 week I was unable to cope with life, totally stressed out about everything, wanting to cry or scream or run away. Zero tolerance towards anyone. After 10 days I realized my mistake and I went back to normal in 24 hrs.
I believe DLPA resulted in very high dopamine as I already have a very slow COMT gene activity for breaking down dopamine.
I now take Endorphigen again but not seeing much effect on sugar cravings this time.
That is quite the reaction she experienced but I’m glad she figured it out so quickly. It’s not uncommon for some folks to react to DLPA like this, feeling more stressed and even anxious. High dopamine, and norepinephrine and epinephrine (so a huge adrenalin rush), related to slow COMT activity could well be the cause.
When Endorphigen (or any of the amino acids) work well initially we continue with trials of higher doses to find the ideal dose. It may also be that a reset is needed after the shift in dopamine.
Rhonda did say she thinks Endorphigen “helped a bit with food cravings.” When it only helps a bit it may be that the dose isn’t high enough or we may need to consider other neurotransmitter imbalances. They can all cause cravings for slightly different reasons: GABA/stress, serotonin/worry or low mood, glutamine/low blood sugar. More on that and the respective amino acids here.
Can GABA be used with DPA?
Ray asks: “Can I use GABA 25mg and also take DPA? Would either/or offset the other?”
My feedback: If someone has low GABA symptoms and GABA helps and they also have low endorphin symptoms and DPA helps then they are absolutely fine to use together and even at the same time. However, I have my clients trial one at a time in order to find the ideal dose and so you know how each one is working
What can I use for my depression and lack of joy, caused by grief?
Vee says she needs something “to get through my grief depression”:
Completely flat, no joy. I always had a calm flat disposition, but now it’s a complete zero. I need my brain to produce some oxytocin so I can like myself, my family and remember all I should be grateful for. I sleep good. I don’t take any meds, and I don’t abuse alcohol. Does tyrosine affect the brain in the way of producing oxytocin?
My feedback: I use DPA/Lidtke Endorphigen for this very purpose. It’s wonderful for grief, depression, lack of joy and the weepiness we see with low endorphins. It also helps with emotional eating that can show up as we try to self-medicate with treats in order to try and feel better.
When the depression also includes being flat, blah and curl-up in bed we use DLPA instead of DPA, or a combination of DPLA/DPA or tyrosine/DPA. Trials of each, one by one, helps you figure out what works best for your unique needs.
And for some folks GABA is helpful as shared by this woman who found GABA allowed her to sit with a feeling of peace and calm most of the time after her mum passed away.
Research does shows a link between dopamine and oxytocin, with oxytocin “emerging as one particular neural substrate that may be influenced by the altered dopamine levels.” Also, for oxytocin support I’d focus on hugs, massage, touch, laughter, making love, yoga, and petting a dog or cat.
DPA and DLPA product options
Products I recommend include Lidtke EndorphiGen (which is DPA) and Pure Encapsulations DL-Phenylalanine (DLPA). You can purchase these from my online store (Fullscript – only available to US customers – use this link to set up an account).
If you’re not in the US, these products are available via iherb: Doctor’s Best D-Phenylalanine (or DPA) and Life Extension D, L-Phenylalanine (or DLPA) (use this link to save 5%).
Additional resources when you are new to using DPA and DLPA, and other amino acids as supplements
As always, I use the symptoms questionnaire to figure out if low endorphins or low dopamine or other neurotransmitter imbalances may be an issue for you.
If you suspect low levels of any of the neurotransmitters and do not yet have my book, The Antianxiety Food Solution – How the Foods You Eat Can Help You Calm Your Anxious Mind, Improve Your Mood, and End Cravings, I highly recommend getting it and reading it before jumping in and using amino acids on your own so you are knowledgeable. And be sure to share it with the practitioner/health team you or your loved one is working with.
There is an entire chapter on the amino acids and they are discussed throughout the book in the sections on gut health, gluten, blood sugar control (this is covered in an entire chapter too), sugar cravings, anxiety and mood issues.
The book doesn’t include product names (per the publisher’s request) so this blog, The Antianxiety Food Solution Amino Acid and Pyroluria Supplements, lists the amino acids that I use with my individual clients and those in my group programs (over and above the few I mentioned above).
If, after reading this blog and my book, you don’t feel comfortable figuring things out on your own (i.e. doing the symptoms questionnaire and respective amino acids trials), a good place to get help is the GABA QuickStart Program (if you have low GABA symptoms too). This is a paid online/virtual group program where you get my guidance and community support.
If you are a practitioner, join us in The Balancing Neurotransmitters: the Fundamentals program. This is also a paid online/virtual program with an opportunity to interact with me and other practitioners who are also using the amino acids.
Wrapping up and your feedback
I do always appreciate questions and feedback like this so keep your questions coming. I do hope my sharing these ones have been helpful to you.
How has DPA or DLPA helped your pain, depression, lack of joy, weepiness, and grief? And has DLPA affected your sleep or made you feel more anxious or stressed?
If yes, which products have helped and do you find swallowed or capsule opened is more effective?
If you’re a practitioner do you use DPA and/or DLPA with clients/patients?
And please let me know if it’s helpful that I’m now including product recommendations and where to get them?
Feel free to share and ask your questions below.