I had to share this with you about my experience with red light therapy. I do not have a Lumebox but purchased a larger device (Red Rush 400) over a year ago from Red Therapy Company after reading a recommendation from Ari Whitten. At the time, I had very painful plantar fasciitis with a heel spur on my left foot that did not respond to an injection.
Because I walk 3-5 miles every day, it was breaking my heart not to be able to walk and I was desperate to find a solution. I placed the bottom of my feet 4-6 inches from the device 10 minutes a day. To my absolute amazement, I noticed the difference in just the first week of using the device and within 2 weeks I was back walking 3-5 miles!
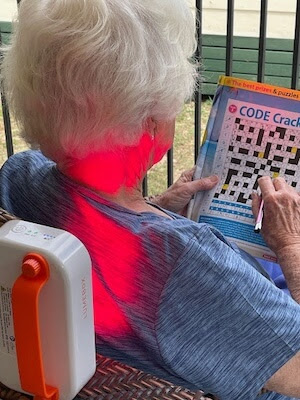
Because we sold our house and moved to Texas recently and are currently living in our 5th wheel RV (hoping to do some traveling) I had not been using my red light device. I developed a very bad pain in my neck and upper back recently (I have degenerative discs) that wouldn’t respond to NSAIDs for 2 weeks.
So I got out my Red Rush 400 and after the first day I started noticing relief which would last about 2 hours. Encouraged, I kept it up 10 minutes a day on each side (front and back) twice a day and within a week the pain was gone. I am sooo amazed how well this works. I’m so grateful to have found this therapy.
Thank you for all you do.
Katherine, a 72 year old woman in the community, sent me this wonderful red light feedback after one of my emails about the Lumebox red light device, and gave me permission to share her success story.
Read on to learn about the research supporting red light therapy for pain, low mood and plantar fasciitis; the two red light devices I own and how I use them, plus the pros and cons of each; amino acids for pain relief and low mood: GABA, tryptophan and DPA; and additional resources if you need guidance using the amino acids.
Red light therapy for pain relief
In case you’re new to red light therapy (or RLT), it’s also known as photobiomodulation (or PBM) or low level laser therapy (LLLT).
This 2021 paper, Low-intensity LASER and LED (photobiomodulation therapy) for pain control of the most common musculoskeletal conditions reports that
There is evidence that photobiomodulation therapy reduces pain intensity in non-specific knee pain, osteoarthritis, pain post-total hip arthroplasty, fibromyalgia, temporomandibular diseases, neck pain, and low back pain.
In this updated paper they confirmed the benefits of red light therapy reporting:
profound biological effects on tissue including increased cell proliferation, accelerating the healing process, promoting tissue regeneration, preventing cell death, anti-inflammatory activity and relief of pain
They also provide good reasons for using opioids at the “lowest effective dose for the shortest period possible”, i.e. adverse effects that include: “poor coordination, sedation, mood swings, depression, and anxiety combined with a dependence on the drugs.”
Red light therapy for low back pain and a mood improvement
In a small study published in 2018, A case control series for the effect of photobiomodulation in patients with low back pain and concurrent depression, the authors report that the participants saw a mood improvement while using red light therapy while doing physical therapy:
This preliminary investigation suggests that an antidepressant effect may result from photobiomodulation (PBM) to the back and thighs in patients with low back pain and concurrent depression.
The authors mention a possible mechanism – NIR and red light used on “large areas of the skin” (like the back and the back of the thighs) “might significantly affect systemic processes such as a slow metabolism, inflammation, and oxidative stress.”
The paper also includes this statement about photobiomodulation being “an FDA-approved treatment for somatic pain …based on the boosting of ATP production by near infra-red (NIR) or red light…” due to mitochondrial support. They also share that “depression has been linked to a decreased level of mitochondrial respiration in blood platelets.”
The authors do acknowledge this was a preliminary finding but what is fascinating is that photobiomodulation may improve mood even when it’s not used directly on the skull.
They also call this a multi-modal approach for pain and low mood, which I fully support i.e. the use of red light therapy in conjunction with dietary changes, exercise, physical therapy, acupuncture and amino acids such as GABA, tryptophan, tyrosine and d-phenylalanine. They don’t mention the amino acids but I share more about these below.
Red light therapy for plantar fasciitis
A meta-analysis presents evidence that red light/photobiomodulation therapy “is an effective treatment modality to reduce pain and improvement of foot function in adults with plantar fasciitis.” They do state that there is a broad discrepancy in the way studies are done for this condition – so you will also see some studies that state it doesn’t help and that it may help pain but other approaches are needed too (which makes sense).
My experience with the Red Rush 400 (panel)
I own the same red light panel – the Red Rush 400 – that Katherine used with success, and I love it. I use it primarily for back and neck pain too – I do 10 minutes at a time when I’m having an issue and also after a weight session at the gym. I’m also learning about the value of doing a daily session at least once a day for better skin health, energy improvement and better sleep.

What I love about this device:
- it covers a large area i.e. from my neck down to my lower back
- it’s very easy to use
- it uses EMF Blocking Cage Technology and has an automatic timer
The negatives are:
- the price (it costs more than the Lumebox)
- it’s very heavy – it hangs on a door but can be easily winched higher or lower as needed
- it’s not portable
If you are wanting to purchase this red light panel, I do have an affiliate account with Red Therapy Co and have arranged $100 off each order if you use the code TRUDYREDTHERAPY at checkout.
I’m sharing about this panel and the Lumebox (below) because I have vetted the products and have first-hand experience with them. I’ve also started receiving other wonderful feedback from my community and will continue to share as more success stories come in.
My experience with the Lumebox device (handheld)
I also own a handheld Lumebox red light device and I love it.
I use it daily, often instead of the panel because it’s so versatile. It comes with us on all our trips and I use it on my feet after a hike or when my restless feet are affecting my sleep (my oxalate issues means I have fickle and tender feet!). I also used it recently on my low back after sitting on bad chairs at a wedding. I’m amazed with the pain relief after just one 10 minute session!
It worked wonders for recovery after a recent fall on my knee – fortunately no broken bones, just bruising and a soft tissue injury. I did use arnica, RICE and amino acids too (GABA and DPA) and saw a physical therapist, but was surprised by how quickly it healed
My hubby uses it more and more and my mom-in-law uses it often on her neck and wrist for osteoarthritic pain.

What I love about this device:
- it’s portable and versatile (and can be used on targeted areas – like on my knee, my feet, neck, jaw etc)
- it’s very easy to use and can be recharged relatively quickly
- it’s low EMF too and also has an automatic timer
- it’s very affordable for what you get
There is only one negative I can think of:
- waiting for it to recharge (only an issue when hubby, mom-in-law are queued up to use it after me)
I also have an affiliate account with Lumebox where you can save $260 off each order when you use my partner link below. No code is necessary and there are other bigger discounts during special sales throughout the year.
I do want to mention that the Red Rush 400 panel and Lumebox handheld device were not actually used in the above studies but participants were exposed to both NIR and red wavelength light, at the same levels that are found in these devices (NIR 850nm and red 660nm).
Amino acids for pain relief and low mood: GABA, tryptophan and DPA
I support a multimodal approach to pain relief and the amino acids are the perfect complement to red light therapy
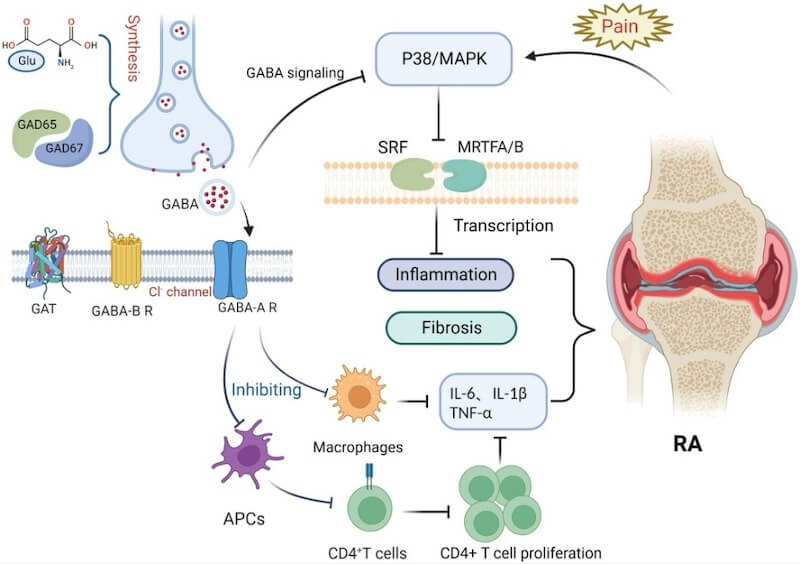
- GABA helps with pain relief when there are spasms and muscle tension (caused by low GABA levels). GABA and GABA/theanine cream can be especially helpful at times.
- Tryptophan helps with pain relief (and low mood) that is caused by low serotonin levels
- DPA (d-phenylalanine) helps with pain relief that is caused by low endorphins. With low endorphins you may also experience emotional pain and weepiness
I’ve blogged extensively about the amino acids and pain so be sure to search the blog with ‘GABA pain’, ‘tryptophan pain’, ‘5-HTP pain’ and ‘DPA pain’ for more about this if you’re new to this aspect. You’ll read many of my own stories about using amino acids for an ankle sprain, rectal spasms/pain, IBS belly pain/spasms and more.
Additional resources when you are new to using amino acids as supplements
As always, I use the symptoms questionnaire to figure out if low GABA or low serotonin or low endorphins and other neurotransmitter imbalances may be an issue.
If you suspect low levels of any of the neurotransmitters and do not yet have my book, The Antianxiety Food Solution – How the Foods You Eat Can Help You Calm Your Anxious Mind, Improve Your Mood, and End Cravings, I highly recommend getting it and reading it before jumping in and using amino acids on your own so you are knowledgeable. And be sure to share it with the practitioner/health team you or your loved one is working with.
There is an entire chapter on the amino acids and they are discussed throughout the book in the sections on gut health, gluten, blood sugar control (this is covered in an entire chapter too), sugar cravings, anxiety and mood issues.
The book doesn’t include product names (per the publisher’s request) so this blog, The Antianxiety Food Solution Amino Acid and Pyroluria Supplements, lists the amino acids that I use with my individual clients and those in my group programs.
If, after reading this blog and my book, you don’t feel comfortable figuring things out on your own (i.e. doing the symptoms questionnaire and respective amino acids trials), if you need serotonin support, the Serotonin QuickStart Program is a good place to start. This is a paid online/virtual group program where you get my guidance on using tryptophan and 5-HTP safely, and community support during 5 LIVE Q&A calls. You can sign up to be notified when the next live launch of this program is happening. We take a deep dive into product options including Lidtke products and others if you’re not able to access Lidtke.
Low GABA can cause physical tension and overwhelm, affect sleep and cause stress eating. If you also have low GABA symptoms, the next step to get help is the GABA QuickStart Program. This is also a paid online/virtual group program where you get my guidance and community support. Another option is the budget-friendly GABA QuickStart Homestudy Program.
Wrapping up and your feedback
I’m thrilled Katherine saw these benefits with red light therapy and I always appreciate feedback from the community and being able to share it on the blog.
Now I’d love to hear from you
Have you used red light therapy with success and which device do you have? How often do you use it?
Have you seen an improved mood with red light therapy too?
And have you used any of the above amino acids to help with pain relief too?
If you’re a practitioner do you recommend red light and amino acids for pain relief? Have you had clients report an improved mood with red light therapy too?