I’m using ox bile (as a supplement) to help counter the effects of dietary oxalates very likely caused by my bile issues and poor fat digestion.
I started with 125 mg ox bile with lunch and dinner and now I’m up to 250 mg at lunch and 375 mg at dinner. Many ox bile products are 500 mg but I decided to start low and go slow and also use an ox bile only product rather than ox bile combined with digestive enzymes.
I don’t know exactly what my liver or gallbladder issues are but suspect low bile production and/or sluggish bile flow.
I have an issue with dietary oxalates and using ox bile confirms my suspicions because I can feel it helping further with symptom reduction (foot and eye pain, and restless legs at night). Because of improved fat digestion, I’m encouraged it’s going to help with longer term bone health (I was recently diagnosed with osteoporosis), immunity, hormone balance and heart health too. I expect better absorption of healthy fats like omega-3 fatty acids, evening primrose oil and fat-soluble vitamins A, E, D and K (and D and K are so important for bone health).
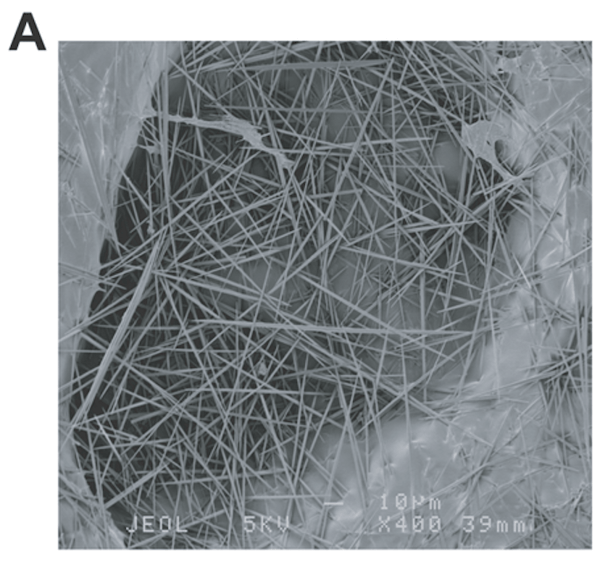
Of course, all this means less oxalate absorption and a reduced impact of the sharp damaging crystals found in medium/high oxalate foods. Oxalates also bind to minerals like zinc, magnesium, and calcium so those mineral deficiencies should shift too.
Read on for a background on oxalate crystal disease, the research on conjugated bile acid replacement therapy (or ox bile supplementation) and oxalate/fat digestion mechanisms, and more about signs of bile issues and solutions. I also share what else I do to mitigate oxalate issues and improve fat digestion, and the ox bile product I am using.
Ox bile increases fat absorption and reduces oxalate absorption
This paper, Conjugated bile acid replacement therapy reduces urinary oxalate excretion in short bowel syndrome, explains that “Soluble oxalate is hyper absorbed by the colon leading to hyperoxaluria and an increased risk for renal calcium oxalate stones and deposits” (and other pain issues – more on that below).
Using ox bile as a supplement (or replacement) with meals “increases fat absorption and thereby decreases calcium fatty acid soap formation and oxalate hyperabsorption.” What does this mean? When fat absorption is improved with ox bile supplements there is more calcium left to bind to excess oxalates in the gut and get rid of them in the stool i.e. less oxalates are absorbed.
I encourage you to read the above paper for a better understanding of the mechanisms.
I do appreciate this team of researchers who have highlighted this approach to help with oxalate issues. Keep in mind I’m experimenting and extrapolating from this single case study of someone with short bowel syndrome and based on what I already know about bile/fat digestion, my own oxalate issues and symptoms of poor bile production/flow (see below).
I don’t have short bowel syndrome but there are a few related studies like this one from the same department, so I feel comfortable experimenting and tracking.
Other pain issues and my pain symptoms caused by dietary oxalates
Keep in mind that the increased absorption of oxalates also causes issues like joint and soft tissue pain, anxiety, restless legs, insomnia, bladder issues, vulvodynia, eye-poking (in autism), thyroid problems, osteoporosis, damage to the heart etc. even when there are no kidney stones. This is not recognized in kidney stone research but is seen extensively in clinical practice.
In 2012 I made the connection between oxalate intake and my excruciating foot pain – a combination of hot-burning-coals-pain and shards-of-glass-pain. The pain has always been worse at night and at its worst I was unable to sleep with severe restless legs. A few years later, I noticed my left eye being affected too, with scratchy discomfort and mild pain. There is also a goopy kind of discharge from the inner part of my eye and burning/redness crystal-like teariness on the outer parts of my eyes.
You can read more about my oxalate story and oxalate crystal disease on this blog – Oxalate crystal disease, dietary oxalates and pain: the research & questions.
It’s more than only ox bile replacement to help with oxalate issues
I say that ox bile helps further because this is a journey I’m on and there are many nutritional approaches that have been helping me over the years. My symptoms have reduced as I do eat mostly low oxalate with some medium oxalate vegetables from time to time, and occasional chocolate or carob (which are high oxalate).
I continue to finesse my use of calcium citrate at bedtime when my symptoms do flare. I am fortunate that I am able to eat cheese so this is another source of calcium for me.
I have pyroluria so I have long used vitamin B6 which is recognized to be helpful for some with oxalate issues. I suspect this may have prevented dumping when I first switched to low oxalate eating.
Signs of low quality bile from Anne Louse Gittleman
These are from her book, The New Fat Flush Plan:
- Queasiness after a fatty meal (impaired bile flow)
- Light-colored or floating stools (lack of bile output)
- Nausea/motion sickness (not enough bile)
- Dry skin and hair (lack of essential fatty acids)
- Constipation (inadequate bile for lubrication)
- Constant feeling of fullness
- Inability to lose weight
- Pain under the right rib cage (reflective pain from the gallbladder)
- Hemorrhoids (congested liver)
- Varicose veins (pressure from constipation due to thickened bile)
- Pain between the shoulder blades (reflective pain from the gallbladder)
- Bloating or gas
- Headache over the eyes (gallbladder meridian passes over this region)
- Bitter taste in the mouth after meals (sign of bile regurgitation)
- History of prescription or recreational drug use (need for more liver and gallbladder support)
- Sensitivities to chemicals
- Easily intoxicated (need for more liver and gallbladder support)
- Fibromyalgia (sign of liver and gallbladder overload)
- Hypothyroidism (sign of deficient bile to stimulate active thyroid hormone in fat cells)
I’m adding these signs/related issues/conditions:
- Fatigue
- Itchy skin
- SIBO/small intestinal bacterial overgrowth
- Osteoporosis
- History of gallbladder attacks or gallstones
- Oxalate issues
In my Anxiety Summit interview with Anne Louise Gittleman she explains what bile is and why it’s so important (read here if you’re new to this).
What I’ve already done to improve my bile production/quality
Here is a quick summary of the advice Anne Louise Gittleman offers, with a note of what I’ve done. I share this to illustrate that I didn’t jump straight to ox bile supplementation/replacement:
- Elimination of food allergies (I’ve done this)
- Addressing low levels of hydrochloric acid or stomach acid (this is not an issue for me)
- Controlling stress (this is ongoing)
- Adding bitter greens to the diet (I do this as much as I can, avoiding medium/high oxalate bitter greens)
- Hot lemon water in the morning (a favorite of the original Fat Flush Plan and something I’ve done for years)
- Adding non-GMO lecithin from soy and sunflowers to your morning smoothie (I don’t do this)
- Using a bile building formula that contains choline, taurine, beet root, inositol and methionine, and pancreatic lipase (I use taurine but can’t use beet root because it’s high oxalate; I did a 2 month trial of a lipase only supplement with no changes; I will likely experiment with choline, methionine and inositol in the near future)
- Using castor oil packs (I plan to do this in the near future)
These are some of the other approaches that can also help:
- Digestive bitters (it does help me and I continue to use it but it’s not enough)
- Toxin removal (I’ve experienced the harmful effects of acute environmental toxin exposure and my daily use of taurine helped. I blogged about this here.)
- Ongoing detox with infrared sauna (I use a Therasage portable sauna)
- Ox bile supplementation/replacement (I chose to use ox bile to be sure it was a bile issue I was dealing with and I did many other interventions first.)
My observations when using ox bile supplementation
I have not had any severe pain flares and have not needed to use extra calcium citrate in the night. The other profound change was a dramatic increase in energy. A few months ago I thought my Lyme was flaring again as I was so exhausted in the afternoons. This exhaustion has dissipated.
In terms of digestive symptoms, I notice less queasiness after a fatty meal like roast chicken with the skin on or a fatty lamb slow cooker stew. The constant feeling of fullness, gas and bloating has improved too. I suspect ox bile is helping with SIBO because it’s antimicrobial. But I can’t be sure since I started berberine 6 months ago and noticed it reduced methane gas production.
I have yet to test out motion sickness on a boat trip but I haven’t been using wristbands in the car and have been fine. I had been having some unusual/new skin itchiness a few months ago and this has now resolved. I do have sensitivities to chemicals but I haven’t noticed any change yet.
I used my stool color as a gauge to whether the ox bile was working – as I increased the dose I noticed it got darker and I have no more floaters. My bowel movements are much easier (more lubrication) and I feel the urge to go more than before.
It will be interesting to see if longer term this helps with improving my bone density. It makes no sense that I have osteoporosis given I’ve been physically active all my life. I highly suspect my bile issues have been a factor since childhood and then got worse during perimenopause Research shows “Gallbladder emptying time is longer during the perimenopausal period.” Unfortunately kidney stones and oxalate issues ramp up in menopause so it’s the perfect storm. I will be discussing all this with my endocrinologist/bone density doctor and ideally do some testing to figure out what the bile issues are (the pancreatic elastase test was fine).
I do track carefully and only make one change at a time so I typically know what improvements I can attribute to what changes.
Ox bile product options


Allergy Research has an Ox Bile 125 mg product and a 500 mg product. You can purchase these from my online store (Fullscript – only available to US customers – use this link to set up an account).
If you’re not in the US, Nutricology has an Ox Bile 125 mg product and a 500 mg product. This is the brand I happen to be using. It can be purchased on iherb (use this link to save 5%).
In conclusion
I’d like to give a shout out to my colleagues… I first learned about oxalates from my dear friend Julie Matthews. Hearing her present at a conference helped me make the connection to my feet pain issues. She introduced me to Susan Owens, oxalate guru and researcher, and the TLO/Trying Low Oxalate group, and now I communicate regularly with them, the TLO moderators and members. And I met Sally K. Norton a few years ago. She is the author of this excellent book, Toxic Superfoods: How Oxalate Overload Is Making You Sick (my Amazon link).
Unfortunately no-one discusses the use of ox bile replacement/supplementation for those of us with oxalate issues and bile issues, and I suspect it’s an under-appreciated tool for those of us who continue to struggle. Hopefully this research and my results starts a discussion on the topic and further interest.
Sally K. Norton does mention a connection in her book: “The immune system has a method for shielding surrounding tissues from oxalate crystals; entrapping them with extruded DNA called a neutrophil extracellular trap (NET). These NETs forming around oxalates may contribute to gallstones and gallbladder “sludge”. If this is the case in my situation, then my lifelong issues with bile were likely made worse by my intake of medium- and high-oxalate foods.
I do hope that me sharing my personal experiments and healing journey helps you or someone you know. Honestly, I could write a book on oxalates and what I’ve learned over the last few years. There is so much to all this and even though it’s a “pain” to be affected like this it is fascinating. I do feel thankful to have dietary and nutritional “solutions.”
The next step for me is looking into and addressing my endogenous oxalate production i.e. oxalates that are produced internally vs oxalates that are ingested. Stay tuned for an update on this.
Do you have oxalate issues together with gallbladder/bile issues/fat digestion issues and how has ox bile supplementation helped you?
Has ox bile helped you with low bile production or sluggish bile – even if you don’t have oxalate issues?
If you’re a practitioner have you used ox bile with your clients or patients?
Feel free to share and ask your questions below.