Do you have dietary oxalate issues (pain, anxiety, insomnia, restless legs, hearing loss, eye issues, unresolved thyroid issues, bladder issues and more) and yet really miss potatoes and even sweet potatoes, both of which are very high oxalate?
I modified a family favorite recipe called Potato Bake (from Pips and my sister) to be a low oxalate option called Butternut Bake.
If you’re new to the dietary oxalate issues you can read more about this below. I’m finding it to be underappreciated as an issue especially in menopausal women when symptoms seems to be more severe in susceptible individuals.
And if you don’t have dietary oxalate issues, you can certainly enjoy this recipe too.
Butternut Bake Recipe (a low oxalate alternative to potato bake)
Ingredients
1 large butternut peeled and sliced thinly
2 cups homemade stock (beef or chicken)
1 cup creme fraiche (or sour cream)
1 teaspoon butter
1 onion (grated)
6 large garlic cloves (grated or crushed in a garlic press)
Salt and pepper
Method
Peel the butternut and slice thinly (½ inch or 1 ¼ cm).
Butter a casserole dish (9×9 inches or 23 x 23 cm) and layer half the butternut slices in the dish.
Sprinkle with salt and pepper, and the grated onion and garlic – spreading it all evenly.
Layer the remaining butternut slices on top.
Bring the creme fraiche to boil and pour in the stock, boil for another minute.
Pour over the butternut.
Bake 180 deg C/350 deg F for 1.5 hours until the liquid has been absorbed by the butternut and the top is golden brown.
Enjoy as a side dish with a serving of quality/organic animal protein like grass-fed beef/lamb or pastured chicken or wild fish and some non-starchy low oxalate veggies such as cauliflower, zucchini or asparagus.
Options
I have not tried it with coconut milk but I’m sure this could be substituted for the creme fraiche.
Low oxalate spices that could be experimented with include: chives, cilantro, basil, lemongrass, parsley, rosemary, ginger and sage.
If you know you don’t have dietary oxalate issues and decide to use potatoes instead, they do need to be cooked in the stock for 10 minutes before layering in the casserole dish. The original recipe calls for 3 large potatoes, sliced.
Some pictures to help as you make this butternut bake
The top image shows the first layer of sliced butternut with grated onion and garlic. And the image below shows the second layer of butternut.


I was very pleased to find some very nice organic creme fraiche which has no added thickeners. The other image below shows the creme fraiche after it’s been boiled in the stock.


The next image shows what the layers of butternut and garlic/onion looks like covered with the creme fraiche/stock mixture i.e. it looks like it may be too much liquid but it really isn’t.

The bottom two images show what it looks like when the Butternut Bake is ready and comes out the oven, and then when it’s been served as a starter or side dish. There is a small amount of thick sauce.


Why consider dietary oxalates as a possible issue?
This blog post is a good one to start with if you’re new to dietary oxalates and the issues they can cause: Oxalate crystal disease, dietary oxalates and pain: the research & questions
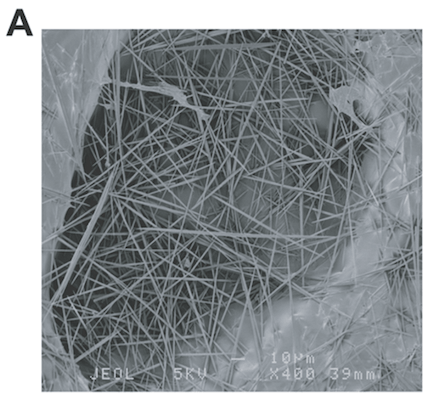
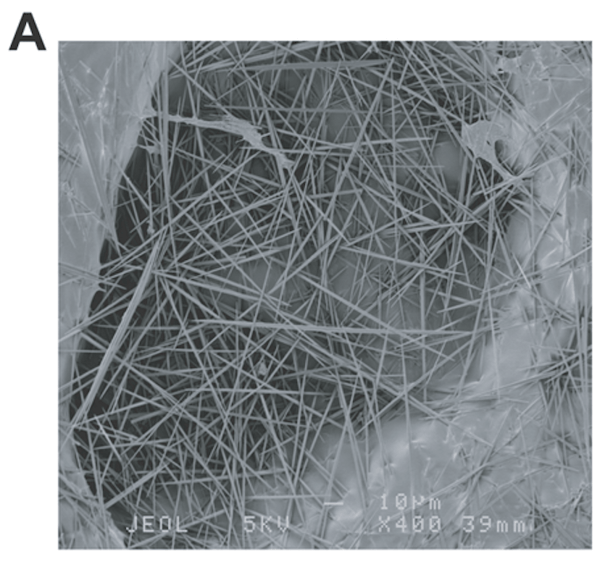
These are the common medium-oxalate and high-oxalate foods that many folks have problems with: nuts, nut-butters and nut-flour (something to watch when eating Paleo or GAPS), wheat, chocolate, kiwi fruit (very high – see the raphides image on the above blog), star fruit (also very high), beets, potatoes, sweet potatoes, legumes, raspberries, spinach and soy.
In the above blog post, I share an overview of oxalates, my pain issues with dietary oxalates (severe foot pain and eye pain), and deeper dive into the condition called oxalate crystal disease (with some of my insights and questions).
The big take-aways are that calcium oxalate crystals are sharp and can cause far reaching harm beyond pain – such as unresolved anxiety, thyroid issues, neurological symptoms, eye issues, hearing loss, bladder issues, headaches, fatigue, insomnia, restless legs, autism symptoms and more; and you can have issues with dietary oxalates and not have kidney disease/kidney stones (although there is very little research supporting the latter).
You may find these oxalate blogs helpful too:
- Waking in the night due to environmental toxins: impacts on the liver, gallbladder and fat digestion (making oxalate issues worse)
- Increased kidney stones in postmenopausal women with lower estradiol levels. What about increased dietary oxalate issues too?
What dietary oxalates issues have you experienced and has a low oxalate diet helped you?
Do let us know if you make this recipe and enjoy it.
Feel free to share a favorite recipe of something you’ve adapted to be low or even medium oxalate.
If you have questions please share them here too.