Today, July 11th, is World Benzodiazepine Awareness Day
This date was designated in recognition of Prof. Heather Ashton’s significant contributions to the benzodiazepine cause over so many decades; together with all of the help she has given to so many people around the world.
In honor of World Benzodiazepine Awareness Day, also called W-BAD I’ve decided to re-release a webinar I did last year: Say NO to Benzodiazepines for anxiety [CLICK THIS LINK TO FIND THE WEBINAR]
Here is an excerpt of the overview from: Say NO to benzodiazepines for anxiety!
Benzodiazepines are a class of psychoactive drugs that work by enhancing the effect of the calming neurotransmitter GABA, and are used to treat anxiety, insomnia, pain, muscle spasms and a range of other conditions. They are widely prescribed, particularly among elderly patients and may even be used off-label with children with autism.
Use of this medication is very controversial. We know long term use leads to tolerance, dependence, and many adverse psychological effects and even physical effects. Short term use is generally considered safe but even using them for 2 – 4 weeks can lead to problems for certain individuals.
This presentation provides an overview of benzodiazepines; when they are used; who they are prescribed to; details about tolerance, dependence, and the many adverse effects; how to taper, including nutritional support during the taper; what to do instead of saying yes to a benzodiazepine prescription in the first place; and additional resources.
Here is one of the benzo stories I share in the webinar:
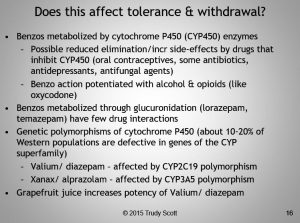
We know that some individuals are much more affected than others when it comes to tolerance and withdrawal. Here are some other possible factors that may affect tolerance and withdrawal:
During season 4 of the Anxiety Summit, Lisa Bloomquist talked about Antibiotic Induced Anxiety – How Fluoroquinolone Antibiotics Induce Psychiatric Illness Symptoms. During this interview she shared how:
People who have gone through benzodiazepine withdrawal before should never take a fluoroquinolone because essentially it can throw people right back into the benzo withdrawal – because it has very similar effects on people’s GABA’s receptors as what happens when people go through benzodiazepine withdrawal.
I would love to see a survey of people who have experienced adverse effects when using benzodiazepines as prescribed or when tapering. Could these be some of the contributing factors?
- Taking Valium/ diazepam and have the CYP2C19 polymorphism (about 10-20% of Western populations are defective in genes of the CYP liver enzyme superfamily)
- Taking Xanax/ alprazolam and have CYP3A5 polymorphism (about 10-20% of Western populations are defective in genes of the CYP liver enzyme superfamily)
- Taking any benzodiazepine and also
- Taking oral contraceptives
- Taking a course of antibiotics
- Taking a course of one of the fluoroquinolone antibiotics
- On an SSRI prescription
- Taking a course of antifungal medications
- Drinking alcohol on a regular basis
- On an opioid such as oxycodone
- Drinking grapefruit juice on a regular basis
For withdrawal/tapering, the best resource I know of is Benzo.org.uk which contains the Ashton Manual. You will need to educate yourself and your doctor and/or find a doctor willing to help you with the adjusted prescription. It does need to be done very very very slowly.
Finding a good support group like Benzobuddies.org is very helpful for many of my clients. Just be aware that this group and some of the other support groups say no to any supplements during the taper process. I find it to be very individualized and have many clients that see great benefit by using GABA, tryptophan, zinc, magnesium and other nutrients. (You can read more about this here: Anxiety and the amino acids overview)
That being said some people tapering can only tolerate very low amounts of the amino acids (like a dab or pinch from a capsule) and some can’t tolerate any supplements and do better with essential oils, yoga, light therapy and dietary changes.
You can find more information on World Benzodiazepine Awareness Day on Benzo Case: Raising Awareness about Benzodiazepine Drugs (widely prescribed for anxiety, stress, sleep, pain and much more…) and additional stories on the World Benzo Awareness facebook page.
World Benzodiazepine Awareness Day was conceived by the acting Chair Barry Halsam, former Chair of Oldham TRANX, and jointly organized by Wayne Douglas, founder of benzo.case.com / benzo-case-japan.com
Please read share so your loved ones are informed and can say NO to benzos!
If you have experienced adverse effects when taking or tapering from benzodiazepines I’d love some feedback on the above possible contributing factors.