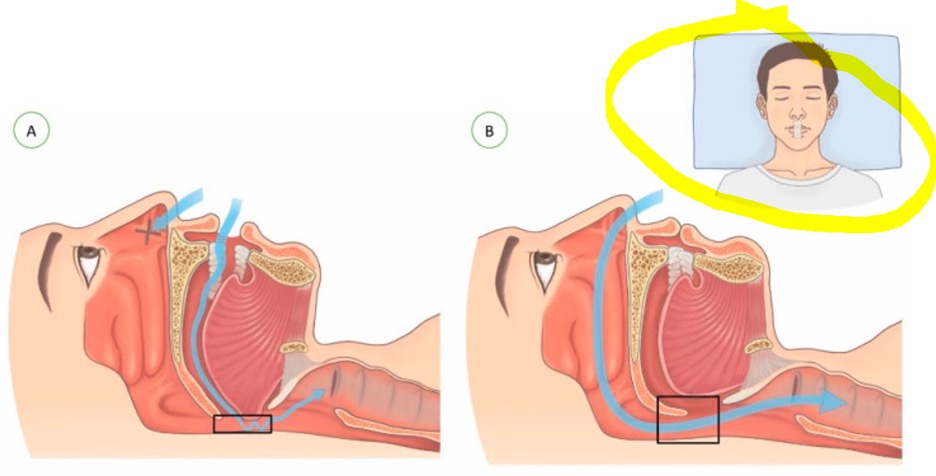
I have had insomnia for years. I have used GABA Calm with good results and also 5-HTP, melatonin and Ambien. Recently I discovered I have mild sleep apnea and have made huge progress in modifying my night awakening.
With my sleep apnea issues addressed, I would like to try to reduce my supplements and the Ambien… but the thought of this causes more anxiety. I feel so dependent on my nightly “cocktail”.
What is the best way to reduce the fear of withdrawal and my nagging brain that tells me I “need” these things?
Many thanks for all the wonderful information you share!
Lynn asked this on one of the blogs and since it’s a common question I’m sharing my feedback in this new blog post. I’m pleased to hear she has discovered sleep apnea is a factor as it’s not always checked and it definitely can cause disrupted sleep and waking in the night.
There is no need to taper amino acids and melatonin but I typically have clients gradually reduce them, one at a time, especially when they are concerned and are not sure how much they may still be helping.
She has a nagging feeling she still needs these supplements, feels dependent on them and feels anxious about stopping. All of this, in conjunction with the fact that stopping a sleep medication such as Ambien can also cause rebound insomnia has me advising a go-slow approach in a situation like this. Also, Ambien does need to be tapered very slowly and under medical supervision, so she would need to keep this in mind too.
A go-slow approach and one amino acid at a time
Lynn may still need one or more of the GABA, 5-HTP and/or melatonin and we don’t want to lose any gains.
As mentioned above, there is no need to taper amino acids and melatonin but I typically have clients gradually reduce them, one at a time, especially when they are concerned and are not sure how much they may still be helping.
I would start with assessing other low GABA symptoms and other low serotonin symptoms and if there are none, start with reducing either GABA or 5-HTP over a few weeks, watching for worsening sleep or other symptoms showing up. She could then do the same with melatonin.
As a reminder, other than sleep issues (with physical tension at night), these are low GABA symptoms: feeling anxious with physical-tension and stiff-and-tense-muscles, overwhelm, feelings of panic, and the need to self-medicate to calm down, often with alcohol but sometimes with carbs and sugary foods. You can also experience anger, rage and agitation, poor focus, intrusive thoughts/overactive brain, spasms, visceral pain/belly pain with IBS and more. You can read the entire list of low GABA signs and symptoms here.
With low serotonin, we see sleep issues with ruminating thoughts and worry (at night too), and fears, phobias, ruminations, obsessing, feelings of panic, perfectionism and lack of confidence, low mood, rage, anger and irritability.
Lynn has a nagging feeling she still needs these supplements, feels dependent on them and feels anxious about stopping. All this is a clue she may still need them or at least need one or more to some extent. Doing a reverse-trial of reducing each one, one at a time, with careful tracking is my approach.
I would tackle the above amino acid and melatonin reduction – if she decides to go ahead with it – only AFTER she has worked with her prescribing doctor on a slow taper on the Ambien. Stopping a sleep medication such as Ambien can cause rebound insomnia/discontinuation syndrome and she may find she does still need nutritional support to tide her over the Ambien taper period. This may be the same as she is currently using or she may even need to adjust upwards on one or more.
Ambien: dependence, withdrawal, rebound insomnia, slow tapering, falls and memory issues
Ambien/Zolpidem “is a non-benzodiazepine receptor modulator primarily used in the …short-term treatment of insomnia aimed at patients with difficulty falling asleep,” increasing “GABA inhibitory effects leading to sedation.”
I seldom see it used short-term i.e. 7 to 10 days. With longer-term use, “this drug has a high potential for overuse and daily dependence” and “withdrawal symptoms may occur if the zolpidem dose is tapered off rapidly or discontinued.”
Other factors to be aware of:
- Complex sleep behaviors can occur after using zolpidem, such as sleep-driving, sleep-walking, and engaging in activities while not fully awake
- Changes in behavior and abnormal thinking have been reported after zolpidem administration. In addition, patients have demonstrated aggressiveness and extroversion uncommon for the person’s usual behavior
- Worsening of depression or suicidal ideation may occur with zolpidem therapy
I encourage you to read the article here and be fully informed.
This 2024 paper supports that “long-term use of Zolpidem may lead to drug tolerance, dependence, rebound phenomena, and withdrawal symptoms, making discontinuation difficult.” Other concerns include: dizziness, headache, falls, and cognitive decline.
Many of the papers published prior to 2023 do not report many of these issues, however awareness is growing. This 2024 paper, Case report: Additional grounds for tighter regulation? A case series of five women with zolpidem dependence from a Brazilian women-specific substance use disorder outpatient service, also reports adverse effects in women such as “memory and social impairment, falls, seizures” and “withdrawal symptoms, including rebound insomnia, social impairment, and craving.”
The authors recommend tighter regulation, stating that: “The surge in zolpidem prescriptions, driven by its perceived safety and low abuse potential compared to benzodiazepines, may lead to a global health issue of dependence.”
Because of much of this it’s important to work with the prescribing doctor on doing a very slow taper under their medical supervision. She may need to adjust her amino acids up during the taper period if her sleep gets worse in the short-term. And then do the taper approach I mentioned at the start of this blog.
With these safety, dependence and withdrawal issues, I would love to see GABA, tryptophan/5-HTP and/or melatonin (and other nutritional and functional medicine approaches), addressing sleep apnea and lifestyle factors/sleep hygiene be considered as the first approach for sleep issues – instead of Ambien/Zolipdem.
Additional resources when you are new to using GABA, 5-HTP and other amino acids as supplements
As always, I use the symptoms questionnaire to figure out if low serotonin or low GABA or other neurotransmitter imbalances may be an issue.
If you suspect low levels of any of the neurotransmitters and do not yet have my book, The Antianxiety Food Solution – How the Foods You Eat Can Help You Calm Your Anxious Mind, Improve Your Mood, and End Cravings, I highly recommend getting it and reading it before jumping in and using amino acids on your own so you are knowledgeable. And be sure to share it with the practitioner/health team you or your loved one is working with.
There is an entire chapter on the amino acids and they are discussed throughout the book in the sections on gut health, gluten, blood sugar control (this is covered in an entire chapter too), sugar cravings, anxiety and mood issues.
The book doesn’t include product names (per the publisher’s request) so this blog, The Antianxiety Food Solution Amino Acid and Pyroluria Supplements, lists the amino acids that I use with my individual clients and those in my group programs.
If, after reading this blog and my book, you don’t feel comfortable figuring things out on your own (i.e. doing the symptoms questionnaire and respective amino acids trials), a good place to get help is the GABA QuickStart Program (if you have low GABA symptoms). This is a paid online/virtual group program where you get my guidance and community support.
If you are a practitioner, join us in The Balancing Neurotransmitters: the Fundamentals program. This is also a paid online/virtual program with an opportunity to interact with me and other practitioners who are also using the amino acids.
Wrapping up and your feedback
I appreciate Lynn for asking this question and want to acknowledge that she is wise to be cautious and have concerns about the best way to tackle this. And she may find she does have a physical dependence on the Ambien.
Have you found that GABA, 5-HTP and/or melatonin helped/helps with your sleep issues?
And is sleep apnea a factor for you too?
And have you been prescribed Ambien and had any of the issues mentioned?
And how have you adjusted your amino acids and other sleep supplements as you’ve tapered your sleep medication?
Feel free to share your feedback and ask your questions below in the comments section.